Our Services -Best Intracytoplasmic Sperm Injection (ICSI) clinic in Pune
ICSI (Intracytoplasmic Sperm Injection) is a specialized IVF technique where a single sperm is injected directly into an egg. At Dr. Shitole's clinic in Pune, ICSI is used for severe male factor infertility and previous poor fertilization with standard IVF.
ICSI Treatment in Pune – Expert Intracytoplasmic Sperm Injection in Kharadi
For men with low sperm count, poor motility, abnormal morphology, or previous vasectomy reversal, standard IVF may result in poor or absent fertilization. ICSI - Intracytoplasmic Sperm Injection - is a game-changing technique that has transformed fertility outcomes for men with severe male factor infertility.
ICIS involves injecting a single sperm directly into the center (cytoplasm) of an egg under a microscope. This technique bypasses the natural fertilization process and dramatically increases fertilization rates even when sperm parameters are severely compromised. At Dr. Rajendra Shitole's clinic in Kharadi,Pune, ICSI is performed with meticulous technique by experienced embryologists under Dr. Shitole's supervision, ensuring optimal outcomes for couples affected by male factor infertility.
What Is ICSI?
ICSI stands for Intracytoplasmic Sperm Injection. The technique involves selecting a single viable sperm under a microscope, drawing it into a specially designed fine needle, and carefully injecting it into the center of a mature egg. This is performed in the embryology laboratory, typically in the evening of egg retrieval.
The development of ICSI in the 1990s revolutionized the treatment of male factor infertility. Before ICSI, men with very low sperm counts, poor motility, or absence of sperm (azoospermia) had no realistic chance of biological fatherhood. ICSI changed this by allowing even a single viable sperm to achieve fertilization.
ICIS is not just injecting any sperm; it requires selecting sperm with appropriate morphology and motility characteristics that suggest viability. This selection process is both an art and a science, requiring expertise and careful observation.


How Does ICSI Differ from Conventional IVF?
In conventional IVF, prepared sperm (millions of them) are placed together with eggs in culture dishes. Fertilization occurs naturally when sperm penetrate the egg's outer membrane and fuse with the egg cytoplasm. This natural process requires adequate sperm numbers and motility.
In ICSI, the entire fertilization process is bypassed. Instead of relying on sperm to find and penetrate the egg, a single sperm is mechanically injected directly into the egg. The egg's natural response mechanisms then activate, and normal development proceeds as if fertilization occurred naturally.
The advantage of ICSI is obvious for men with poor sperm parameters. When conventional IVF results in zero or minimal fertilization due to inadequate sperm, ICSI can achieve normal fertilization rates (70-80%), dramatically increasing the chance of embryo development and pregnancy.
However, ICSI adds cost to the IVF cycle (typically ₹15,000-₹25,000 additional) and introduces a slight additional step in the laboratory process. Therefore, ICSI is recommended selectively - for cases where male factor infertility would otherwise result in poor fertilization outcomes.
Who Benefits from ICSI?
ICSI is indicated for several male factor conditions. These include oligospermia (low sperm count - less than 15 million sperm per milliliter), asthenospermia (poor sperm motility - less than 40% motile), teratospermia (abnormal sperm morphology - less than 4% normal forms), combination male factor (multiple parameters abnormal), azoospermia (absence of sperm in ejaculate), and ejaculation dysfunction where sperm is retrieved surgically.
ICIS is also indicated when previous IVF resulted in zero or poor fertilization, even if semen parameters were borderline. Sometimes the egg's ability to be fertilized is the issue, not just the sperm, and ICSI helps in these situations.

ICIS is not recommended for every couple. In cases of male factor infertility with borderline but acceptable sperm parameters, and in cases where the female partner has good fertility markers, the doctor may recommend attempting conventional IVF first before resorting to ICSI. However, in cases of severe male factor, ICSI is recommended immediately.
The ICSI Procedure: Step-by-Step
For couples choosing ICSI, the IVF process is largely similar to conventional IVF up to the point of fertilization. The differences are in the laboratory procedure.
Preparation of Sperm for ICSI
On the day of egg retrieval, sperm is collected (by ejaculation or surgical retrieval in cases of azoospermia). The sample is processed to separate sperm from other components. For men with very low counts, special techniques may be used to concentrate available sperm. The goal is to identify viable sperm that can be used for injection.
In men with zero sperm in the ejaculate (azoospermia), sperm may be retrieved surgically from the epididymis (PESA - Percutaneous Epididymal Sperm Aspiration) or testis (TESE - Testicular Sperm Extraction). These procedures can be performed under local anesthesia. If sperm retrieval is planned, this is discussed and scheduled in advance.
Selection of Sperm for Injection
Under a high-magnification microscope (typically 400x magnification), the embryologist carefully observes sperm and selects those with characteristics suggesting viability. These typically include normal morphology, some degree of motility, and appropriate size and shape. The selection process is meticulous because injecting abnormal sperm may result in fertilization failure or abnormal development.
For some cases, special techniques like IMSI (Intracytoplasmic Morphologically Selected Sperm Injection) use even higher magnification (6000x) to select sperm with optimal morphology. This is particularly valuable in cases of teratospermia (abnormal morphology) or previous ICSI failure.
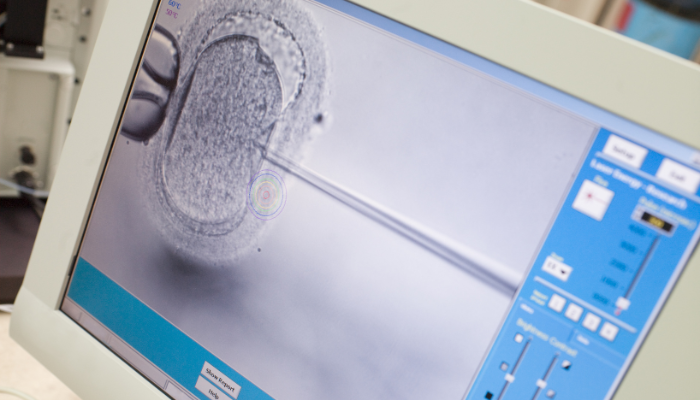
The Injection Procedure
Each selected sperm is drawn into a fine injection needle (immobilization pipette). Under microscopic view, the embryologist positions a mature egg in a holding pipette. The injection needle, containing the selected sperm, is carefully guided through the egg's outer membrane (zona pellucida) and into the cytoplasm. The sperm is released into the egg, and the needle is withdrawn.
This procedure is performed for each mature egg in the cycle. If 10 mature eggs are retrieved, approximately 10 injections are performed. The entire ICSI procedure typically takes 1-2 hours. After injection, eggs are returned to culture medium in an incubator.
The technical skill required for ICSI cannot be overstated. Poor injection technique can damage the egg and prevent fertilization. At Dr. Shitole's clinic, the embryologists performing ICSI are highly trained and experienced, minimizing technical failures and maximizing fertilization success.
Fertilization Assessment and Embryo Development
The morning after ICSI, fertilization is assessed by observing for the presence of two pronuclei in each injected egg - evidence that the sperm nucleus has successfully fused with the egg nucleus and fertilization has occurred. Normal fertilization rates with ICSI are 70-80%, compared to 50-70% with conventional IVF in non-male-factor cases.
Following fertilization, embryo development proceeds as with conventional IVF. Embryos are monitored daily, transferred on day 3 or day 5-6 depending on quality and number, and hormone support is provided. The remainder of the IVF cycle is identical.
ICSI Success Rates and Outcomes
Success rates with ICSI depend on several factors: the woman's age (the most important factor), ovarian reserve, embryo quality achieved after fertilization, and the specific cause of male factor infertility.
For men with severe male factor who would have zero fertilization with conventional IVF, ICSI may transform a completely unsuccessful cycle into a successful one. Success rates in such cases reflect the female partner's age and ovarian reserve, not the male factor limitation.
For couples with borderline male factor and female age less than 35, ICSI success rates typically range from 35-45% per cycle. For women 35-37, rates are 25-35%. For women over 40, rates are 15-25%. These are comparable to or slightly better than conventional IVF in non-male-factor cases, because ICSI ensures optimal fertilization.
Some studies suggest that ICSI may slightly increase miscarriage rates in some cases, which is why ICSI is used selectively only when male factor justifies it. However, recent large studies have not confirmed this concern, and ICSI outcomes appear equivalent to conventional IVF when fertilization is successful.
ICSI for Azoospermia: Surgical Sperm Retrieval
For men with azoospermia (complete absence of sperm in the ejaculate), ICSI combined with surgical sperm retrieval offers hope for biological fatherhood. There are two main types of azoospermia: obstructive (where sperm is produced but blocked from ejaculation due to vasectomy or absence of vas deferens) and non-obstructive (where the testicles don't produce sperm due to genetic, hormonal, or other issues).
In obstructive azoospermia, sperm can typically be retrieved surgically. PESA (Percutaneous Epididymal Sperm Aspiration) or TESA (Testicular Sperm Aspiration) are minimally invasive outpatient procedures performed under local anesthesia. A small needle is inserted into the epididymis or testicle, and sperm is aspirated. Retrieved sperm is then used for ICSI.
In non-obstructive azoospermia, TESE (Testicular Sperm Extraction) or TESE with microsurgical techniques (micro-TESE) may retrieve sperm in about 50-60% of cases. The testicle is examined under magnification to identify regions with spermatogenesis, and tissue from these regions is carefully excised. Single sperm found in these tissue samples can be used for ICSI.
Dr. Shitole coordinates these procedures and manages ICSI cycles for azoospermia, offering men who otherwise might have no chance of biological parenthood a realistic opportunity.
Cost of ICSI Treatment
ICSI adds cost to an IVF cycle. While standard IVF at Dr. Shitole's clinic in Pune costs ₹1-2.5 lakh per cycle, adding ICSI typically increases the cost by ₹15,000-₹25,000. If surgical sperm retrieval is needed (for azoospermia), an additional ₹5,000-₹15,000 is added.
Despite the additional cost, ICSI represents excellent value for men with severe male factor infertility. For men who would otherwise have no chance of biological parenthood, the additional investment in ICSI is a small price for the opportunity to father a biological child.
Dr. Shitole's Approach to ICSI
Dr. Rajendra Shitole's expertise in ICSI is grounded in his training and experience. His fellowship in IVF and endoscopy from Ruby Hall Clinic included extensive laboratory training in sperm selection and injection technique. His subsequent practice managing male factor cases has refined his judgment in ICSI application.
Dr. Shitole recommends ICSI only when it's truly indicated - based on semen analysis, previous fertilization failures, or the specific diagnosis. He doesn't recommend ICSI to every couple with male factor, as this would increase costs unnecessarily. Instead, he individualizes the recommendation, explaining the rationale and discussing alternatives.
For couples where ICSI is recommended, Dr. Shitole works with experienced embryologists to maximize fertilization success and embryo quality. The combination of proper patient selection, technical expertise, and high-quality laboratory conditions results in good outcomes for men with male factor infertility.